Coming Soon!
The 50-State Health Freedom Index
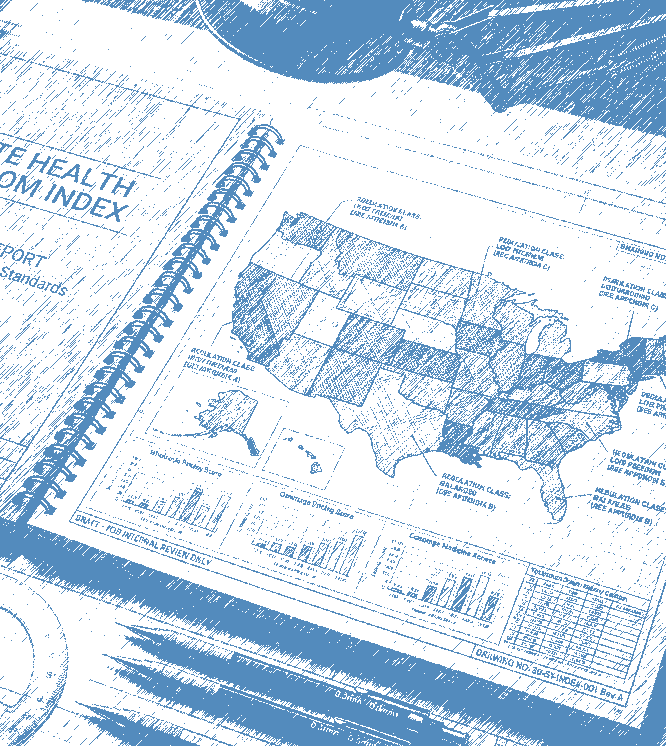 We are excited to announce that the Center for Modern Health, in partnership with the Knee Regulatory Research Center at West Virginia University, is preparing to release the 2026 Health Freedom Index—a new 50-state ranking of health and healthcare freedom across the United States.
We are excited to announce that the Center for Modern Health, in partnership with the Knee Regulatory Research Center at West Virginia University, is preparing to release the 2026 Health Freedom Index—a new 50-state ranking of health and healthcare freedom across the United States.
The report will be officially unveiled during a session at the State Policy Network's Annual Meeting on Wednesday, August 26. We will post the full report, including all scores and rankings, and users will be able to download the data spreadsheet.
To get an invitation to download the report as soon as it is available, subscribe to our newsletter.
"Junk insurance" is a catch-all term for health plans that do not meet conventional standards of comprehensive coverage. But the coverage that one can get through mechanisms such as health sharing ministries, short-term plans, catastrophic plans, and high-deductible plans can serve different needs and budgets. This should cause us to ask questions about who should decide which forms of coverage have a place in the market.

Continue reading...
We trust doctors with our health and our lives, yet that trust seems to dissipate when that very same doctor owns the facility in which care is delivered. Why? Doctors themselves have spent decades portraying business success as incompatible with medical professionalism. Until physicians defend entrepreneurship as an asset to patient care, opposition to physician-owned hospitals will unfortunately persist.

Continue reading...
Just as other features of American healthcare obscure the true cost of care, hospital cross-subsidization hides the economics of individual services. By masking which services are profitable and which are not, our system distorts prices and hides useful signals. Importantly, it also complicates reform. Legislative efforts to introduce competition attract pushback from incumbent hospitals that need profits from some departments to sustain other departments.

Continue reading...
Mark Cuban's Cost Plus Drugs proves that bypassing insurers can dramatically lower costs through direct, transparent pricing. To that extent, it should be praised. But true disruption requires challenging not just PBMs and insurers, but also the assumption that comprehensive insurance is the best way to pay for everyday care. Until that idea changes, efforts to improve affordability and transparency will remain constrained.

Continue reading...
President Adams signed into law an act requiring that twenty cents per month be deducted from the wages of private merchant sailors and paid into a federal fund for their medical care. It is sometimes described as America’s first health insurance mandate, but in truth it is not strong evidence that the founders would approve of today's calls for government involvement in healthcare.

Continue reading...
The No Surprises Act eliminated surprise medical bills by replacing balance billing with a government-run arbitration process. But without transparent, market-based healthcare prices, arbitrators have no objective basis for determining fair payment rates. Lasting reform requires restoring price transparency and expanding direct-pay healthcare markets that allow real price discovery and consumer choice.

Continue reading...
Section 6001 of the Affordable Care Act effectively prevents new physician-owned hospitals from participating in Medicare, dramatically limiting their growth. The debate over repeal reveals deeper questions about corporate versus physician ownership, subsidy-seeking, taxpayer interests, and whether government policies have distorted healthcare markets in ways that undermine genuine competition and patient choice.

Continue reading...
Medicaid fraud is highly concerning, but the federal crackdown on the issue misses a deeper problem: rules that punish honest providers and disempower patients. Instead of relying solely on AI and aggressive enforcement, policymakers should expand cash-pay options, permit parallel practice, and give patients greater control over healthcare dollars to build a system that rewards integrity.

Continue reading...
The current FDA review process generates a single decision that everyone must abide by. What if instead we adopted a more permissive approach for drugs entering the private market, and stricter review (including cost) for drugs seeking coverage by public payers? This acknowledges the difference between private and public, and would expand patient choice while protecting taxpayers and reducing political pressure on regulators.

Continue reading...
When patients lose the power to shape healthcare with their own dollars, profits stop serving patients and start serving regulations. From Certificate of Need laws to prior authorizations, government interventions often distort incentives, while freer models like Direct Primary Care and Cost Plus Drugs show how profits can align with patient interests.

Continue reading...
Americans are often told that healthcare corporations restrict patient choice and drive up costs in pursuit of profit. But the deeper problem is the dominance of comprehensive health insurance itself. By financing routine care through insurance, the system disconnects patients from prices and limits their ability to reward affordable care. Expanding alternatives to comprehensive health insurance could restore competition and affordability.
Continue reading...
Concerns about English proficiency often arise in debates over reforming the way that we allow foreign-trained physicians to apply for a medical license. Evidence shows they perform comparably to U.S. graduates, with safeguards minimizing risks. Published research does not show a systematic link between limited English proficiency and worse outcomes, suggesting such concerns should not block reform efforts.

Continue reading...