Health Policy Predictions: 2nd Annual Survey
Which changes are most likely to occur in the next five years?

View/Download [PDF]
Rhoads, J. "Health Policy Predictions: 2nd Annual Survey" Center for Modern Health. December 2025.
Introduction
Of all the things that could shift in U.S. health policy over the next five years, which changes are most plausible? Will national health spending continue its upward climb and edge past 20 percent of GDP? Might long-discussed reforms to the tax treatment of employer-sponsored coverage finally materialize? How likely are we to see significant growth in direct primary care, cash-pay surgical centers, or legally sanctioned supervised injection sites (i.e., overdose prevention centers)? And could an alternative pathway for drug approval emerge alongside or in place of the current FDA process? Even rough, informed expectations about these possibilities can help policymakers, scholars, clinicians, and advocates decide where to focus their attention and energy.
Forecasting is, of course, a humbling activity. Many researchers have noted how poorly individual experts tend to perform when asked to predict future political events.1 Experts often cling to their priors, reinterpret new information to fit their outlook, and struggle to update their beliefs in real time.2
However, even though individual experts often get it wrong, there is evidence that pooling independent judgments can produce more reliable forecasts. It's not that there's some sort of "collective brain"; that's not how it works. Rather, what produces the wisdom-of-crowds effect is that idiosyncratic errors tend to cancel out when many people offer independent estimates, so long as the group is not swayed by a shared bias or a single dominant voice. Classic demonstrations include guessing the number of objects in a jar to estimating the height of famous landmarks such as the Eiffel Tower.3 In forecasting, we can leverage this to get a better "guesstimate" about the likelihood of something happening.
This report presents the results of a survey exercise aimed at estimating the likelihood of 28 potential developments in U.S. health policy over the next five years. The participants were a diverse group of people who either follow or work in healthcare in one way or another, including experts and non-experts. The propositions spanned a wide landscape of issues, from national spending trends and insurance reforms to the growth of direct-to-consumer care models and evolving state and federal policies on drug use and access to services.
The goal is not to claim clairvoyance, but to offer a structured snapshot of how knowledgeable observers currently assess the direction of U.S. health policy. With this being our second time fielding this survey, we are able to report not just this year's findings but also indicate the differences between this year's results and last year's results.
As U.S. healthcare continues to adapt to technological change, political pressures, and ongoing debates about its future, we hope these findings provide useful perspective for anyone engaged in the work of shaping, studying, or navigating American healthcare.
Methods
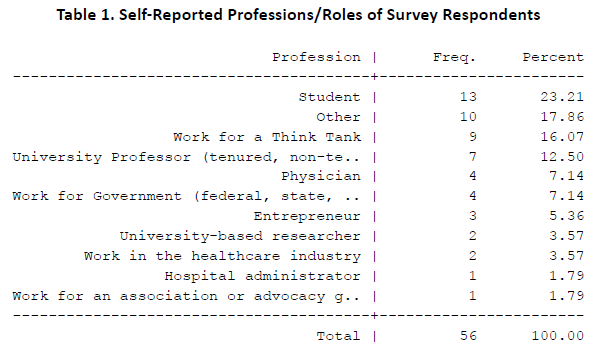
We obtained responses from 56 individuals with knowledge about healthcare to rate the likelihood that various health policy changes will happen in the next five years. Respondents were recruited through convenience sampling, starting with known health policy leaders from think tanks, physicians, and academia, and other sources. To add a light "Delphi" element to this exercise, we invited all of the respondents from the previous year to take the survey, and to all invitees we also shared a link to the previous year's report. Thus, individuals were able to give their responses independently yet also see the previous "round" of predictions if desired.
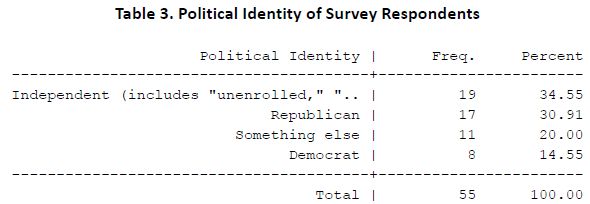
Five pure opinion questions—separate from the prediction questions—were presented to survey takers in order to gauge their "free-market friendliness." These were not screening questions; there was no litmus test in order to participate in this survey. These questions were asked to understand the ideological skew of the respondent pool, as a check against overgeneralizing results later on. Five questions were coded into one composite variable with a possible range of 5 to 25. On that scale, where 5 is extremely unfriendly to markets in healthcare, and 25 is extremely friendly to markets in healthcare, the average respondent in our survey scored about 18 with a standard deviation of about 6. This means our respondent pool was generally, but not exclusively, composed of individuals friendly to markets.

As the following table shows, despite respondents generally being friendly to free-markets in healthcare, they were diverse in terms of political identity.
The survey instrument was fielded using Qualtrics software. No monetary or gift incentive was offered to respondents in exchange for taking the survey.
There were 28 prediction questions in total, grouped into four sets of seven questions for the sake of on-screen visual neatness and user-friendliness. Within each group of 7 questions, the order of the questions was automatically randomized from one survey taker to the next by the Qualtrics software. We asked respondents to offer predictions on the same propositions this year as last year, making it possible to report the longitudinal difference.
Respondents were allowed to skip questions if they did not have a strong enough opinion to warrant making a prediction, but most respondents answered most of the prediction questions in the survey. They were reminded to provide probabilities based on what they thought would happen, not what they would like to see happen. Questions were answered at a high rate. The 28 prediction questions received an average of exactly 50 predictions (out of a possible 56), with the range on that measure being 38 to 56. (If every respondent answered every question, the average number of predictions would be 56.)
Results
Results were cleaned and tabulated using Stata statistical software. The consolidated findings are shown below, where "N" is the number of observations; "Median" is the median probability; and Δ is the difference between this year's Median probability and last year's probability.
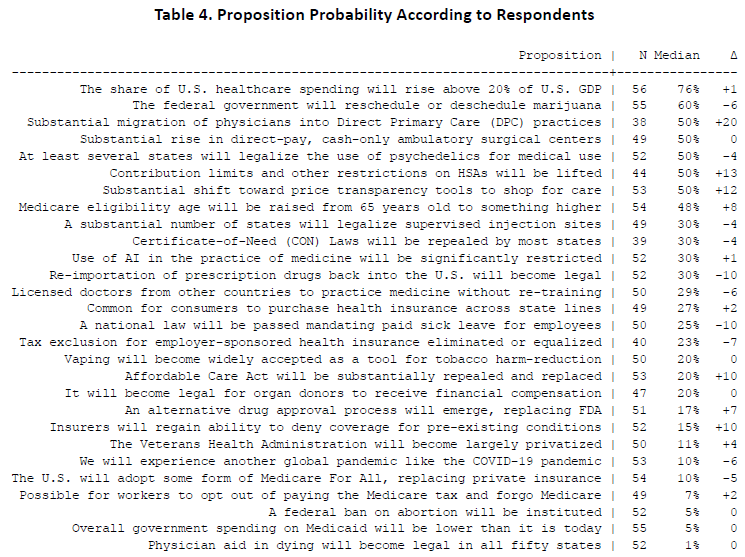
In the rest of the report, we showcase each proposition one at a time, providing a summary and context about the issue and reporting the specific results for that proposition. A "turnip plot" is provided for each proposition, illustrating the distribution of the responses. In these plots, each dot represents one respondent's prediction.
The propositions are presented in the order in which they were numbered in our survey instrument.
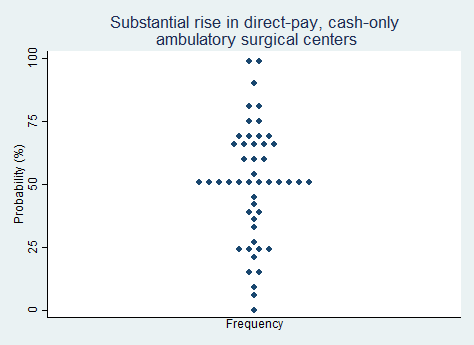
Proposition 1.
"There will be a substantial rise in the number of direct-pay, cash-only ambulatory surgical centers."
2025 Median prediction: 50% prob (n = 49)
2024 Median prediction: 50% prob (n = 48)
Unlike traditional healthcare facilities that rely heavily on insurance reimbursements, direct-pay ambulatory surgery centers (ASCs) operate on a cash-based model. One key part of the value proposition is that they offer patients clear and upfront pricing for medical procedures. This approach eliminates the administrative complexities of billing third-party payers, reducing overhead costs and increasing efficiency. This model empowers patients to shop for care based on quality and cost, thereby fostering competition among providers.
Recent years have seen a gradual but notable shift towards direct-pay models, driven by dissatisfaction with opaque pricing in traditional healthcare systems and rising out-of-pocket costs for insured patients. The growth of high-deductible health plans has further incentivized patients to seek cost-effective alternatives. However, state regulations—including some that require ASCs to accept all payers or that require amenities such as a 24-hour emergency department—present barriers to growth for direct-pay ASCs across the United States. Respondents in our survey are roughly split over the question of whether direct-pay ASCs will become substantially more common in the next five years.
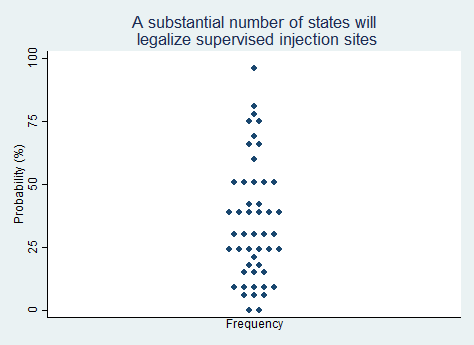
Proposition 2.
"A substantial number of states will legalize supervised injection sites (a.k.a. overdose prevention centers)."
2025 Median prediction: 30% prob (n = 49)
2024 Median prediction: 34% prob (n = 40)
Supervised injection sites (SISs), also known as overdose prevention centers (OPCs), are facilities where individuals can use pre-obtained drugs under the supervision of trained staff. These sites aim to reduce harm by preventing overdose deaths, minimizing the spread of infectious diseases such as HIV and hepatitis C, and by connecting individuals to addiction treatment and social services. Advocates argue that they are a pragmatic response to the opioid crisis, emphasizing public health over punitive measures. Evidence from international examples including Canada, Europe, and Australia, suggests that this approach can improve health outcomes without increasing drug use or crime in surrounding areas.
In the United States, the debate over SISs and OPCs has been contentious. Opponents cite concerns about enabling and normalizing drug use, as well as legal concerns. Federal law, particularly the Controlled Substances Act, has historically been a barrier. As public opinion shifts toward treating addiction as a health issue rather than a criminal one, some states and municipalities are exploring legislative changes that could allow pilot programs. Respondents in our survey are very split over whether we can expect a noticeable increase in states embracing these approaches in the next five years.
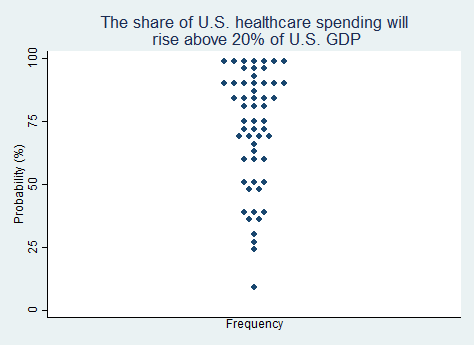
Proposition 3.
"The share of U.S. healthcare spending will rise above 20% of U.S. GDP (currently about 18%)."
2025 Median prediction: 76% prob (n = 56)
2024 Median prediction: 75% prob (n = 51)
Currently, healthcare spending accounts for approximately 18% of U.S. GDP. Among OECD countries, this is several percentage points higher than the next highest countries (Germany and France). Factors driving high spending include rising utilization from an aging population, rising cost of medical technologies and pharmaceuticals, rising administrative complexity, and expansive government programs and involvement in the sector.
The prospect of healthcare spending rising above 20% of GDP underscores deep systemic challenges. Policymakers and experts worry about the implications for federal and state budgets, employer-sponsored insurance, and household financial stability. At the same time, growing prevalence of chronic disease may exacerbate the upward trajectory of costs. Debates about reform often center on cost control measures, such as payment model innovations, regulatory interventions, and investments in preventive care. The question remains whether payment model reforms, investments in preventative care, or other ideas will curb spending growth. Respondents in our survey appear confident that spending will exceed 20% of GDP in the next five years.
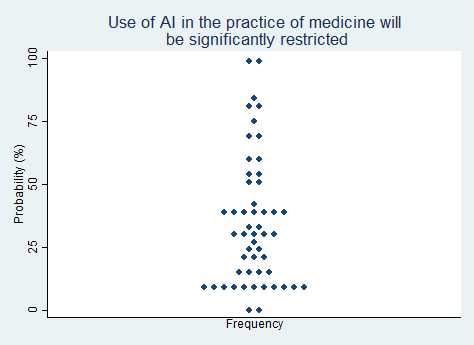
Proposition 4.
"Use of artificial intelligence in the practice of medicine will be significantly restricted."
2025 Median prediction: 30% prob (n = 52)
2024 Median prediction: 29% prob (n = 49)
The integration of artificial intelligence (AI) into medical practice is an area of great potential and great debate. Prominent applications for AI-powered tools include imaging diagnostics, personalized medicine, predictive analytics, and administrative automation. However, the rapid adoption of AI has also raised concerns about patient safety, algorithmic bias, data privacy, and accountability for errors. These concerns could lead to government restrictions on its use in medicine.
Critics argue that without rigorous oversight, AI systems could perpetuate or amplify existing disparities in healthcare outcomes. Questions also exist about liability, for example whether responsibility lies with the clinician, the AI developer, or the institution. Legal clarity on some of these issues is needed. Regulatory agencies, such as the FDA, have taken steps to establish frameworks for evaluating and approving AI tools, but it is not clear whether additional restrictions are to be expected—and if so, what they will entail. Respondents in our survey continue to be optimistic that AI will not be significantly restricted in the next five years.
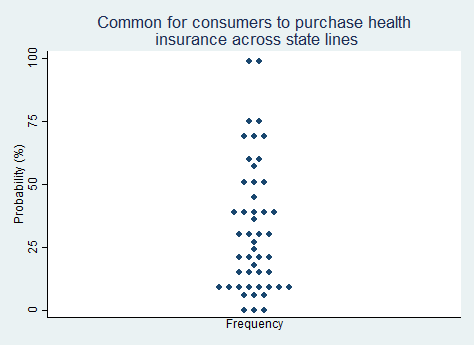
Proposition 5.
"It will become relatively common for states to allow consumers to purchase health insurance across state lines."
2025 Median prediction: 27% prob (n = 49)
2024 Median prediction: 25% prob (n = 47)
Allowing consumers to purchase health insurance across state lines has been a recurring proposal in U.S. health policy discussions. Advocates argue that this policy could enhance competition among insurers, lower premiums, and expand consumer choice. They see it as enabling individuals to shop for more tailored plans offered from insurers in states with fewer coverage mandates. Critics, on the other hand, contend that allowing cross-state sales could lead to a "race to the bottom," where insurers gravitate toward states with the least stringent regulations, potentially undermining consumer protections and fragmenting risk pools.
Interest in the idea of purchasing health insurance across state lines is often strongest among free-market advocates, and is not always supported by the insurance companies themselves, who cite operational challenges, such as integrating provider networks across states, as barriers. Some states have passed laws permitting cross-state insurance sales, but the results have been lackluster, perhaps due to policy inertia. Opinion is split on the likelihood of this idea gaining momentum in the next five years, with a majority expressing pessimism.
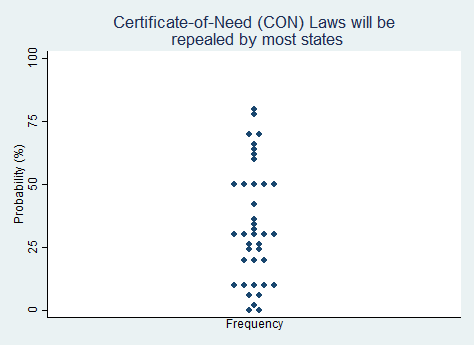
Proposition 6.
"Certificate-of-Need (CON) Laws will be repealed by most of the states that currently still have them."
2025 Median prediction: 30% prob (n = 39)
2024 Median prediction: 34% prob (n = 47)
Certificate-of-Need (CON) laws require healthcare providers to obtain state approval before expanding facilities, adding new services, or acquiring certain types of medical equipment. Originally enacted in the 1970s to control healthcare costs and prevent duplication of services, these laws started to lose favor in the 1980s, leading some states to repeal their CON laws. Today, CON laws remain in place in about two-thirds of U.S. states, and their scope and requirements vary widely.
Critics contend that CON laws stifle competition, limit patient choice, and protect entrenched interests, such as large hospital systems, from new market entrants. Empirical evidence suggests that CON laws do little to contain costs or improve access. Repealing CON laws generally increases competition, which is why industry incumbents are often willing to defend the laws. During the COVID-19 pandemic, some states temporarily waived CON requirements to meet surging healthcare demands, prompting calls for permanent deregulation. Respondents to our survey are split and lean negative on the question of whether most states will repeal their CON laws in the next five years.
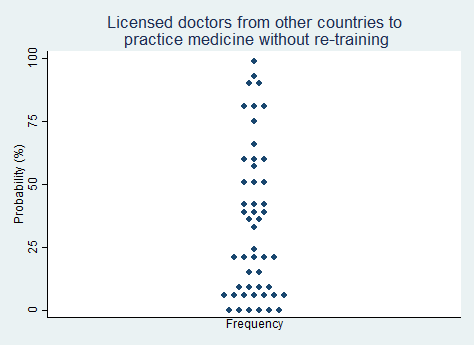
Proposition 7.
"A substantial number of states will allow licensed doctors from other countries to practice medicine without repeating their residency/fellowship training."
2025 Median prediction: 29% prob (n = 50)
2024 Median prediction: 35% prob (n = 48)
The United States has long relied on internationally trained physicians to address workforce shortages, particularly in underserved and rural areas. However, foreign-trained doctors must typically undergo extensive retraining, including repeating their residency or fellowship programs, before they can practice medicine in the U.S. Although this arrangement ensures adherence to American medical standards, it is a time-consuming and costly barrier for professionals who are already licensed and practicing in their home countries.
Advocates for streamlining licensure argue that the status quo is sheer economic protectionism for incumbent doctors. Recognizing the qualifications of foreign-trained doctors without requiring them to repeat training would increase physician supply, helping to alleviate physician shortages and attracting more international talent. While some states have begun experimenting with more flexible licensing pathways or bridging programs, widespread adoption of these policy changes are uncertain. Respondents in our survey are split on whether a substantial number of states will relax their restrictions, with most predicting that states will not shift in that direction.
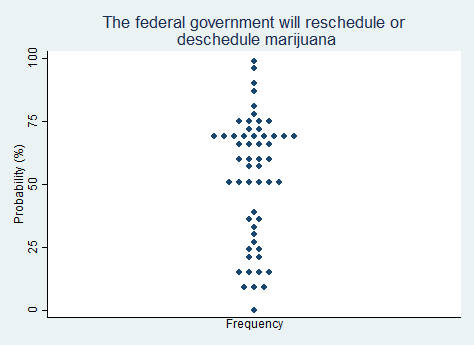
Proposition 8.
"The federal government will reschedule marijuana to a less strict classification under the Controlled Substances Act, or deschedule it altogether."
2025 Median prediction: 60% prob (n = 55)
2024 Median prediction: 66% prob (n = 47)
The classification of marijuana as a Schedule I substance under the Controlled Substances Act (CSA) places it alongside drugs like heroin and LSD, which is supposed to be reserved for substances with a high potential for abuse and no accepted medical use. This classification has been a barrier to cannabis research, medical use, and legalization efforts. It also conflicts with the growing acceptance of marijuana for recreational and medicinal purposes. At least 24 states have legalized recreational marijuana, and about 40 states permit its medical use, creating a stark contrast between federal and state policy.
Rescheduling marijuana to a less strict category, such as Schedule II or III, would recognize its medical potential but still leave it subject to federal regulation. Descheduling it entirely would remove marijuana from the CSA, treating it similarly to alcohol or tobacco. Advocates for reform argue that rescheduling or descheduling would resolve the state-federal conflict and promote research for medical and health uses. Opponents warn of potential public health risks, including increased use among adolescents. In 2024, President Biden issued a directive to reschedule cannabis from Schedule I to Schedule III, but the change was never finalized. Respondents in our survey are split but tend to believe that rescheduling or descheduling will happen in the next five years.
Proposition 9.
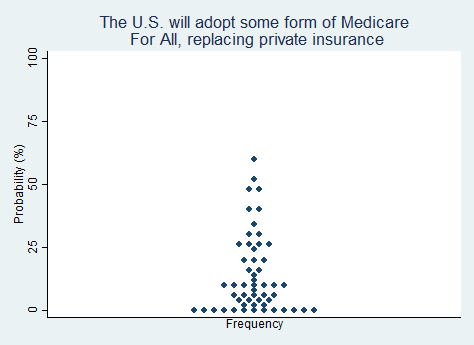
"The U.S. will adopt some form of Medicare For All, replacing private insurance."
2025 Median prediction: 10% prob (n = 54)
2024 Median prediction: 15% prob (n = 51)
The idea of "Medicare for All" envisions a healthcare system in which the federal government serves as the only payer, effectively replacing most private health insurance. Long associated with political figures such as Bernie Sanders in the U.S. Senate and Pramila Jayapal in the U.S. House of Representatives, Medicare for All draws inspiration from healthcare models in countries such as Canada and the United Kingdom, promising reduced administrative costs, and universal coverage through the elimination of premiums, deductibles, and co-pays.
Implementing Medicare for All would entail a major transformation of the U.S. healthcare system, requiring significant tax increases and an increase in government control over the lives of Americans. Once a fringe idea of the political left, consistent promotion of the idea in Congress and among activists has made the idea more politically palatable to some. The vast majority of respondents in our survey appear to regard the likelihood of the U.S. going the route of Medicare for All as unlikely in the next five years.
Proposition 10.
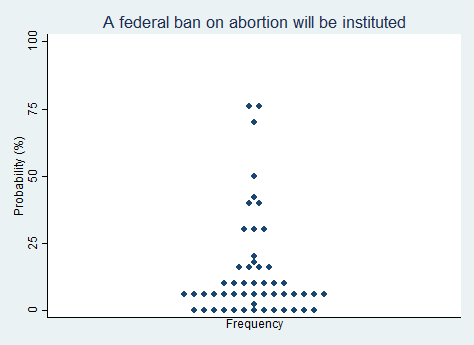
"A federal ban on abortion will be instituted."
2025 Median prediction: 5% prob (n = 52)
2024 Median prediction: 5% prob (n = 47)
The issue of abortion remains one of the most polarizing topics in U.S. politics. Since the Supreme Court's 2022 decision in Dobbs v. Jackson Women's Health Organization overturned Roe v. Wade, the regulation of abortion has largely been left to individual states. This has created a patchwork of laws across the country, with some states enacting near-total bans while others have moved to expand or protect access in various ways, including via so-called shield laws. In the post-Dobbs landscape, many observers wonder whether the federal government might next institute a nationwide abortion ban.
Advocates for a federal abortion ban argue that it would create consistency across states and reflect the moral opposition that many Americans have to abortion. Opponents view a federal ban as an infringement on individual rights and on states' ability to govern themselves as they see fit. Pursuing a ban would require significant support in Congress, and would likely face constitutional challenges. By and large, respondents in our survey believe it is very unlikely that a federal ban on abortion will be instituted anytime in the next five years.
Proposition 11.
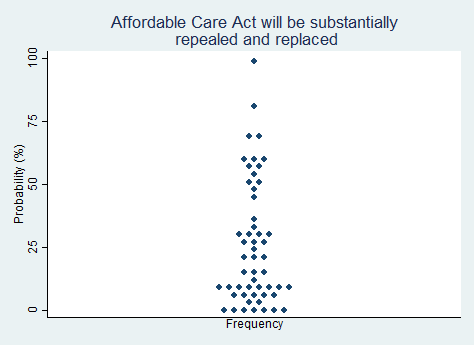
"The Affordable Care Act will be substantially repealed and replaced with something else."
2025 Median prediction: 20% prob (n = 53)
2024 Median prediction: 10% prob (n = 49)
The Affordable Care Act (ACA), enacted in 2010 on a strictly partisan vote, represents one of the largest overhauls of the U.S. healthcare system in decades. Its key provisions include expanding Medicaid eligibility, preventing insurers from denying coverage to individuals with pre-existing conditions, and providing individuals with subsidies to purchase health insurance. While the ACA has reduced the number of uninsured individuals in the country, it has faced persistent criticism for increasing premiums, imposing mandates, and causing insurers to narrow their physician provider networks.
Efforts to repeal and replace the ACA reached a peak in 2017 but ultimately fell short in Congress with Senator John McCain's iconic "thumbs-down" vote. Since then, some aspects of the ACA, such as the individual mandate penalty, have been weakened or eliminated, while other parts have remained intact. As of this writing, the enhanced subsidies for ACA plans are set to expire at the end of 2025. Advocates of full ACA repeal argue that the ACA is unsustainable and overly restrictive. Opponents argue that repeal could jeopardize insurance coverage for millions of Americans. Respondents in our survey see it as very unlikely that the ACA will be substantially repealed and replaced in the next five years.
Proposition 12.
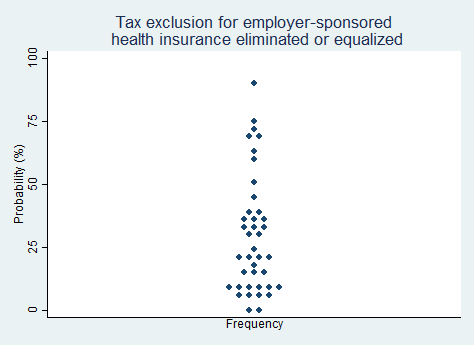
"The tax exclusion for employer-sponsored health insurance will be either eliminated or extended to insurance that individuals buy outside of an employer arrangement."
2025 Median prediction: 23% prob (n = 40)
2024 Median prediction: 30% prob (n = 45)
The tax exclusion for employer-sponsored health insurance (ESI) is one of the most enduring—and some believe notorious—features of the U.S. healthcare system. Roughly 165 million people, or about 60% of people under age 65, get their health coverage through their employer in one way or another. Under this policy, the value of health insurance premiums paid by employers is excluded from employees' taxable income, providing a substantial benefit to those who buy coverage this way.
Proposals for reform generally fall into two categories: eliminating the exclusion altogether or extending similar tax advantages to individuals who purchase health insurance outside of employer arrangements. Advocates for reform argue that these changes would level the playing field for individual insurance markets, spur new innovation in those areas, and finally discourage the purchase of excessive coverage. Opponents argue that altering the exclusion could destabilize employer-sponsored coverage or lead to higher taxes generally. Respondents in our survey tend to predict that the tax exclusion will not be substantially changed in the next five years.
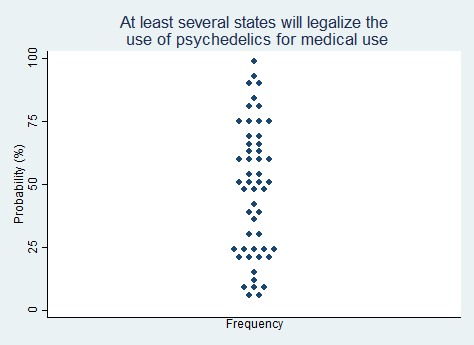
Proposition 13.
"At least several states will legalize the use of psychedelics (e.g., LSD, psilocybin) for medical or therapeutic use."
2025 Median prediction: 50% prob (n = 52)
2024 Median prediction: 54% prob (n = 48)
The movement to legalize psychedelics for medical and therapeutic purposes has gained significant momentum in recent years. Substances like psilocybin (the active compound in "magic mushrooms") and LSD are being studied for their potential to treat mental health conditions such as depression, anxiety, PTSD, and substance use disorders. Early clinical research has shown promising results, leading to increased interest from medical professionals, policymakers, and advocacy groups. Psilocybin, in particular, has already been decriminalized or legalized for therapeutic use in Oregon and Colorado, as well as in certain municipalities.
Advocates for legalization argue that psychedelics represent a potential paradigm shift in mental health treatment, offering hope for patients who have not responded to conventional therapies. They emphasize the importance of regulation and oversight to ensure safety and efficacy. Critics express concerns about the long-term effects, potential for misuse, and challenges of integrating psychedelics into the existing medical framework. If psychedelics do become legal in more places, questions about insurance coverage will surely follow. Respondents in our survey are roughly split on the question of whether the trend in legalization of psychedelics will continue over the next five years, with a slight majority predicting that it will continue.
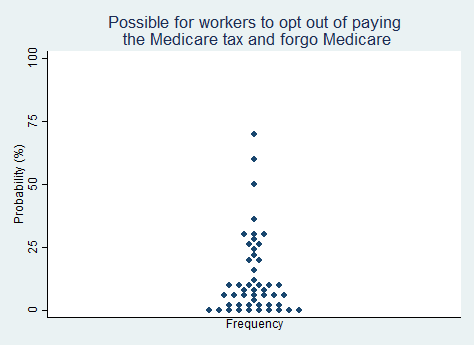
Proposition 14.
"It will become possible for workers to opt out of paying the Medicare tax in exchange for permanently forgoing the option to enroll in Medicare when they get older."
2025 Median prediction: 7% prob (n = 49)
2024 Median prediction: 5% prob (n = 47)
Medicare is a federal health insurance program for people aged 65 and older, as well as for those with certain disabilities, End-Stage Renal Disease (ESRD), or ALS. Under the current system, all workers contribute 1.45% of their earnings to Medicare, with an additional 0.9% tax on high-income earners. These contributions are used to fund the Medicare program, which provides healthcare benefits to individuals over the age of 65.
In a fully free society, there would be no place for such a major government program, but considering how firmly ensconced Medicare is at present, it is hard to imagine a politically practical path toward abolition. One option is to pursue this policy goal very gradually over many years, allowing workers to opt out of paying the Medicare tax today in exchange for permanently forgoing Medicare coverage when they reach retirement age. Supporters of this approach argue that it would give workers greater control over their finances and allow them to allocate funds toward alternative retirement savings or private insurance. This proposal is occasionally floated by think tank analysts but rarely discussed by office-holding politicians. In our survey, respondents rated the chance of the U.S. adopting a genuine opt out option for Medicare in the next five years as extremely unlikely.
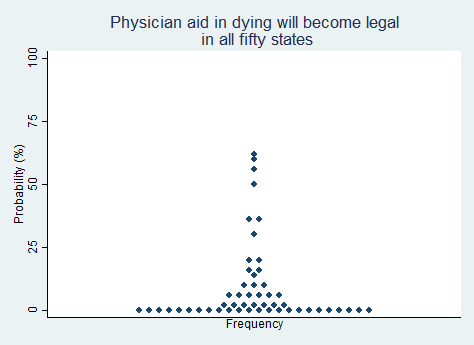
Proposition 15.
"Physician aid in dying (a.k.a. physician-assisted suicide) will be made legal in all fifty states."
2025 Median prediction: 1% prob (n = 52)
2024 Median prediction: 1% prob (n = 45)
Physician aid in dying (PAD), sometimes called medical aid in dying (MAID) or physician-assisted suicide (PAS), involves a medical professional providing a terminally ill patient with the means to end the patient's life, usually through a prescription for lethal medication. In 11 states plus DC, laws allow patients with a terminal diagnosis and a certain prognosis to request assistance in dying. Although details can vary, patients typically must meet strict criteria, such as a mental competency assessment and a waiting period, to ensure that they are making an informed and voluntary decision.
The debate over whether PAD should be legal involves a range of ethical, legal, and medical considerations. Advocates argue that allowing PAD respects individual autonomy and provides a compassionate option for those suffering from unrelievable pain or a loss of dignity. Some opponents contend that legalizing PAD could lead to vulnerable individuals feeling pressured to end their lives. Others—particularly those with religious beliefs—argue that PAD undermines societal values around the sanctity of life. While public opinion has shifted in favor of PAD in recent years, achieving widespread acceptance would require overcoming significant challenges. Respondents to our survey indicated that they believe it is extremely unlikely that PAD will be made legal in all fifty states in the next five years.
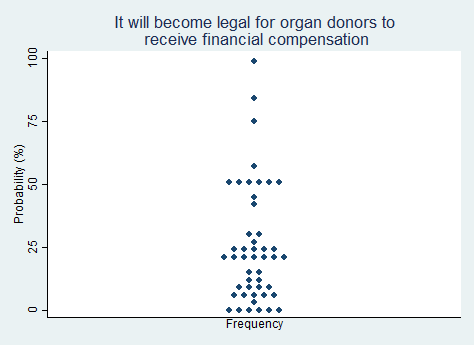
Proposition 16.
"It will become legal for organ donors to receive financial compensation."
2025 Median prediction: 20% prob (n = 47)
2024 Median prediction: 20% prob (n = 45)
In the United States, organ donation is currently governed by the National Organ Transplant Act (NOTA) of 1984, which prohibits financial compensation for organ donors. Under this system, organ recipients are typically responsible for covering the medical expenses of their organ donors (meaning that the recipient's insurance will typically cover the costs of the donor's evaluation, surgery, and post-operative care), however additional compensation is not allowed. While this framework has helped maintain ethical standards in organ donation, it has also led to chronic shortages of available organs, with thousands of individuals waiting for transplants each year.
Allowing financial compensation for organ donation is one way to increase the supply of organs and reduce the transplant waiting list. Supporters have proposed that donors could receive direct payments or tax incentives. Opponents raise ethical concerns, fearing that compensation could lead to exploitation of vulnerable populations and introduce new health inequities. Most respondents in our survey believe it is unlikely that it will become legal for organ donors to receive financial compensation in the next five years.
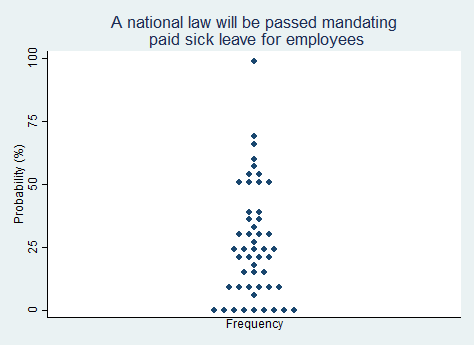
Proposition 17.
"A national law will be passed mandating paid sick leave for employees."
2025 Median prediction: 25% prob (n = 50)
2024 Median prediction: 35% prob (n = 50)
The issue of paid sick leave has been a focal point of labor policy discussions in the United States, particularly as the COVID-19 pandemic highlighted the vulnerabilities of workers without access to paid sick days. Such policies are largely determined at the state or local level, with roughly a dozen states mandating such a benefit, and federal law addressing unpaid leave under the Family and Medical Leave Act (FMLA) in certain situations. Many employers provide paid sick leave voluntarily to higher-wage employees. Workers in lower-wage and gig economy jobs generally do not get paid sick leave.
Advocates for a national paid sick leave law argue that such a policy would improve public health by reducing presenteeism (workers coming to work while sick). It could also provide economic security for workers, especially those with children or other caregiving responsibilities. Opponents of a national mandate contend that it would impose significant financial burdens on businesses, and is a local work benefit decision best left to employers. Respondents in our survey do not think it is likely that a national law will be passed mandating paid sick leave in the next five years.
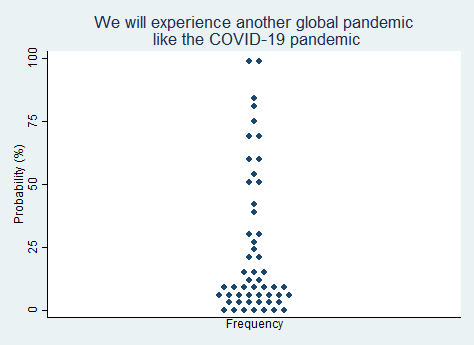
Proposition 18.
"We will experience another global pandemic that is roughly the magnitude of the COVID-19 pandemic."
2025 Median prediction: 10% prob (n = 53)
2024 Median prediction: 16% prob (n = 47)
The possibility of another global pandemic, comparable in scale and impact to COVID-19, remains a topic of significant concern and preparation within the global health community. COVID-19, caused by the SARS-CoV-2 virus, highlighted global health vulnerabilities and the profound social and economic disruptions that pandemics can cause. Infectious disease experts agree that when it comes to future pandemics, the question is not whether it will happen again but when.
Global health organizations, including the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC), continue to monitor emerging infectious diseases, but there is no consensus on the precise timing or magnitude of the next pandemic. Some experts argue that increased investment in early detection systems and global coordination could help mitigate the risks, while others hold that the complex interplay of biological and social factors make pandemic prediction and prevention exceedingly difficult. Respondents in our survey gave a wide range of probabilities to the question of whether we will experience another global pandemic like COVID-19 in the next five years, but most predict it will not happen.
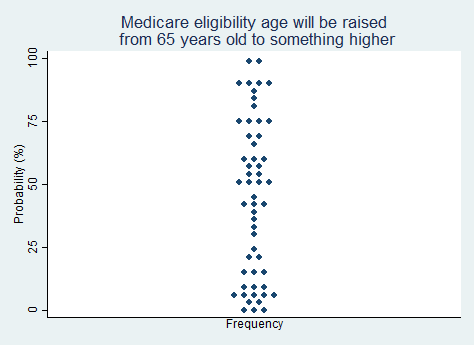
Proposition 19.
"The age of eligibility for Medicare will be raised from 65 years old to something higher."
2025 Median prediction: 48% prob (n = 54)
2024 Median prediction: 40% prob (n = 51)
Medicare is the federal health insurance program for individuals aged 65 and older. As the U.S. population continues to age, with Baby Boomers entering retirement and life expectancy rising, the financial sustainability of Medicare has come under increasing scrutiny. Currently, Medicare is funded through payroll taxes and premiums, but the growing number of beneficiaries relative to the working-age population poses significant challenges to the program's long-term solvency. In response, some policymakers have proposed raising the age of eligibility for Medicare from 65 to 67 or 70, as a means of improving the program's fiscal health.
Delaying the point at which beneficiaries begin drawing from the system could help reduce the strain on Medicare's trust funds. Opponents of this proposal argue that it would place additional financial burdens on older Americans, particularly those who are in poor health or unable to work past 65. Some also argue that it is unfair to "change the rules in the middle of the game." This debate highlights the ongoing tension between controlling federal spending and ensuring the existence of a program that people have come to rely upon, which some consider a kind of forced dependence. Respondents in our survey are almost evenly split on whether they think the Medicare eligibility age will be raised in the next five years.
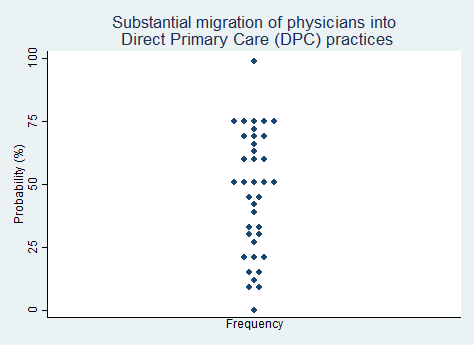
Proposition 20.
"There will be a substantial migration of physicians into Direct Primary Care (DPC) practices."
2025 Median prediction: 50% prob (n = 38)
2024 Median prediction: 30% prob (n = 48)
Direct Primary Care (DPC) is a model of healthcare delivery that bypasses traditional insurance billing to create a direct doctor-patient relationship. In this model, patients typically pay a monthly membership fee, which covers most primary care services, including routine exams, simple tests, and preventive care. DPC has gained traction in recent years as an alternative to insurance-based models, offering physicians greater autonomy over their practices and more time to spend with patients. Proponents argue that DPC reduces administrative burdens, allows for more personalized care, and helps address the growing demand for primary care services.
DPC offers physicians a way to regain control over their work-life balance and reduce dependence on third-party payers, however it can be challenging for physicians to leave the comforts of working in a large health system or group practice to "go independent." A certain entrepreneurial spirit and risk tolerance is needed to make the switch. Regulatory barriers, such as statutes that threaten to subject DPC practices to insurance requirements, are slowly coming down, but still present in some places. Respondents in our survey were split over the likelihood that DPC will grow substantially over the next five years, after having been much more pessimistic on this proposition in last year's survey.
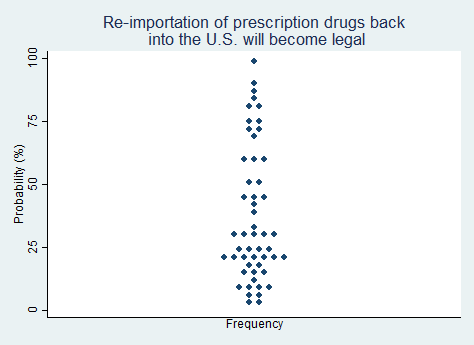
Proposition 21.
"Re-importation of prescription drugs back into the United States from other countries where they are sold more cheaply will become legal."
2025 Median prediction: 30% prob (n = 52)
2024 Median prediction: 40% prob (n = 49)
The issue of re-importing prescription drugs from other countries has been a long-standing topic of debate in U.S. healthcare policy. Prescription drugs in the U.S. are often sold at higher prices than in other developed countries due to factors including patent protections and the negotiation power of governments in foreign markets. As a result, many Americans seek cheaper alternatives by purchasing medications from countries like Canada, where drug prices are significantly lower. Allowing re-importation would mean that U.S. residents, pharmacies, and wholesalers could bring these less expensive drugs back into the U.S. legally, bypassing high domestic prices.
Advocates argue that re-importation is a type of freedom of association. Opponents of re-importation express concerns about the safety and legitimacy of drugs purchased abroad (i.e., the drugs could be counterfeit), and argue that drug manufacturers have the right to set and enforce different prices in different markets. Opponents also argue that re-importation could disrupt the domestic pharmaceutical market and undermine innovation. Current federal law prohibits the reimportation. The state of Vermont tried to establish a reimportation program but was prevented from doing so by the federal government. Most of the respondents in our survey are skeptical that re-importation of prescription drugs will become legal in the next five years, but some believe this could happen.
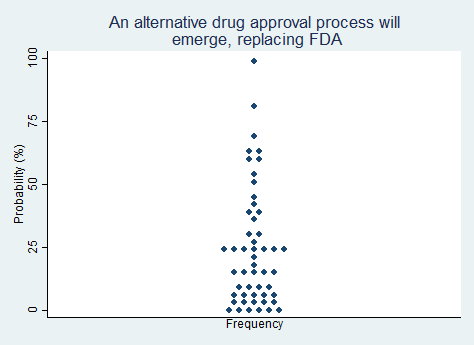
Proposition 22.
"An alternative drug approval process will emerge, replacing some or all of the Food and Drug Administration (FDA)."
2025 Median prediction: 17% prob (n = 51)
2024 Median prediction: 10% prob (n = 46)
The U.S. Food and Drug Administration (FDA) is the central authority overseeing the approval of new drugs. The FDA's approval process is time-consuming, costly, and slow. Indeed, it can be argued that having an approval process at all constitutes a type of unjustified "preventive law." These criticisms have sparked discussions around the possibility of alternative drug approval mechanisms, such as a decentralized model or one that relies on private certifying bodies. These could potentially replace some or all of the FDA's current functions.
FDA supporters argue that more subtle reforms are sufficient. Programs such as the FDA's Breakthrough Therapy designation and the accelerated approval pathway for certain drugs have helped to make it somewhat easier for promising treatments to reach the market faster. Opponents would prefer to see the function of the FDA turned over to competing private organizations or possibly reformed to be similar to the less centralized European Medicines Agency (EMA). A vigorous debate over whether to substantially replace the FDA could take form. Most respondents in our survey do not believe it is likely that an alternative drug approval process will emerge in the next five years.
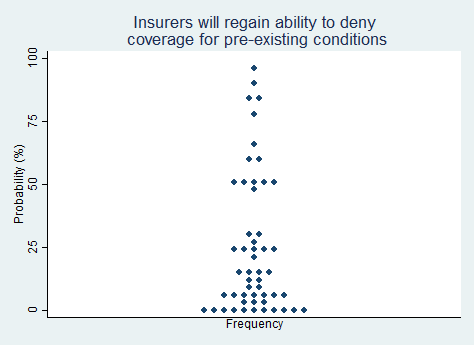
Proposition 23.
"Health insurance companies will regain the ability to deny coverage to people with pre-existing conditions."
2025 Median prediction: 15% prob (n = 52)
2024 Median prediction: 5% prob (n = 48)
Prior to the passage of the Affordable Care Act (ACA), insurance companies could deny coverage or charge higher premiums to individuals with pre-existing conditions. Although this state of affairs made it possible for some people with serious medical needs to be left uninsured, it kept premiums affordable for many other people by preserving the role of insurance as a protection against an unexpected, unintended future risk.
The ACA changed this by prohibiting insurers from denying coverage or charging higher premiums based on pre-existing health conditions. Restoring insurance to a pre-ACA state would once again make insurance conceptually coherent and it would reduce premiums for many, but the ACA provision regarding pre-existing conditions has been popular and few political figures on either side of the aisle today are willing to advocate for its reversal. The vast majority of respondents in our survey rate the likelihood of this change taking place in the next five years as very low.
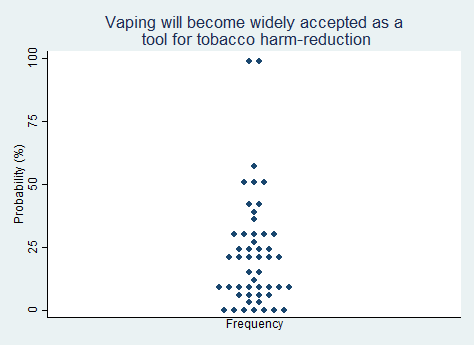
Proposition 24.
"Vaping (i.e., use of e-cigarettes) will become widely accepted as a positive tool for tobacco harm-reduction."
2025 Median prediction: 20% prob (n = 50)
2024 Median prediction: 20% prob (n = 46)
E-cigarettes heat a liquid containing nicotine and flavoring agents to produce a vapor that is inhaled, without the combustion process that occurs with regular cigarettes. Vaping, or the use of e-cigarettes, has become a charged topic in public health discussions. Whether vaping becomes widely accepted as a positive tool for harm reduction depends on future research, public health advocacy, and future regulatory decisions. It is perhaps the arch example of a harm-reduction versus abstinence debate.
Proponents of vaping argue that it provides a less harmful alternative to smoking, potentially helping smokers reduce their exposure to harmful tar and chemicals. As such, vaping could be a valuable tool for tobacco harm reduction for some individuals. Critics, however, raise concerns about the long-term health effects of e-cigarettes, given that the products are relatively new and research on their safety is ongoing. Critics also raise concerns about the rising popularity of vaping among adolescents and non-smokers, which could lead to a new generation becoming addicted to nicotine. Respondents in our survey largely do not believe that vaping will gain acceptance as a tobacco harm reduction tool in the next five years.
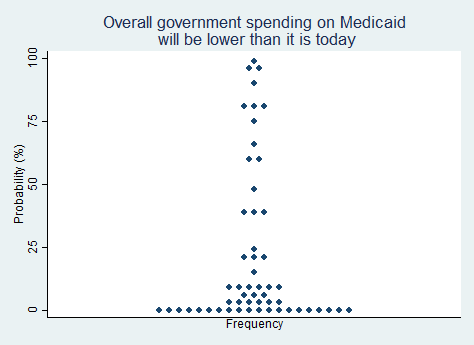
Proposition 25.
"Overall government spending on Medicaid will be lower than it is today."
2025 Median prediction: 5% prob (n = 55)
2024 Median prediction: 5% prob (n = 46)
Medicaid is the joint federal and state program that provides healthcare coverage for low-income individuals and families. The federal government covered about 69 percent (about $620 billion) of the cost of the program in 2023, and states contributed the rest. Medicaid spending has increased in recent years as more people have become eligible for the program, particularly in states that chose to expand Medicaid under the ACA. This has led to concerns about the financial sustainability of the program.
Proposals to lower government spending on Medicaid include transforming Medicaid into a block grant program, where states would receive a fixed amount of funding and have more flexibility in managing their Medicaid programs. Others have suggested requiring beneficiaries to pay more in premiums or co-pays or imposing work requirements to reduce enrollment. These approaches are generally supported by most Republicans and opposed by most Democrats. The trajectory of Medicaid spending will depend on political decisions and ongoing debates about policy priorities. Although some of the respondents in our survey believe that spending cuts are likely, most of the respondents in our survey predict that overall government spending on Medicaid will be higher in five years than it is today.
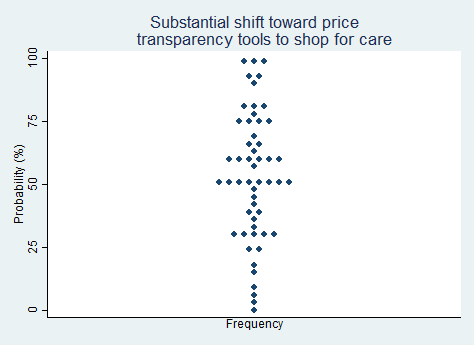
Proposition 26.
"There will be a substantial shift toward patients and consumers using price transparency tools to shop for care and procedures."
2025 Median prediction: 50% prob (n = 53)
2024 Median prediction: 38% prob (n = 50)
Price transparency in healthcare has become an area of focus in U.S. health policy, as consumers increasingly seek ways to manage the rising costs of medical care. Healthcare prices—at least for areas outside of cosmetic procedures—are opaque, to say the least. Patients are often unaware of the true cost of care until after they have received treatment, leaving consumers unable to compare prices or make informed decisions. In recent years, some consumer advocates and private companies have tried to improve price transparency by enabling patients to "shop" for care by comparing prices across different healthcare providers.
With more accessible pricing information, we would likely get greater competition among providers, which would help to drive down costs. However, almost no market incumbents see this as being in their interest. Price opaqueness benefits the seller, not the buyer. If early innovators succeed at introducing price transparency tools, disruption could follow, potentially reshaping how patients navigate the healthcare market. Respondents in our survey are evenly split on the question of whether price transparency tools will substantially catch on in the next five years.
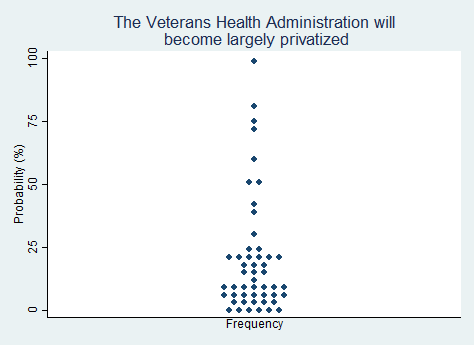
Proposition 27.
"The Veterans Health Administration will become largely privatized."
2025 Median prediction: 11% prob (n = 50)
2024 Median prediction: 7% prob (n = 43)
The Veterans Health Administration (VHA) is the largest integrated healthcare system in the United States. It provides medical care to over 9 million veterans around the country through a network of hospitals, clinics, and other facilities, as well as plays a role in functions such as graduate medical training. As a tax-funded, integrated system, it is structurally perhaps most similar to Britain's National Health Service (NHS). Whether the VHA should remain as it is or be privatized is a subject of ongoing debate. VHA has an annual budget of approximately $68 billion.
Advocates for privatizing VHA argue that privatization would improve access to care, reduce wait times, and offer veterans more choices in where they receive treatment. Opponents of privatization express concerns about the potential loss of the unique benefits the VHA provides, such as specialized services for veterans, continuity of care, and a focus on military-related health issues. They also express concern about the financial viability of turning over veteran care to an expensive and opaque private world of healthcare delivery. Whether VHA will become privatized will depend on political debates about spending, and the attitudes that veterans have about the care they receive. The respondents in our survey do not think it is likely that VHA will become privatized in the next five years.
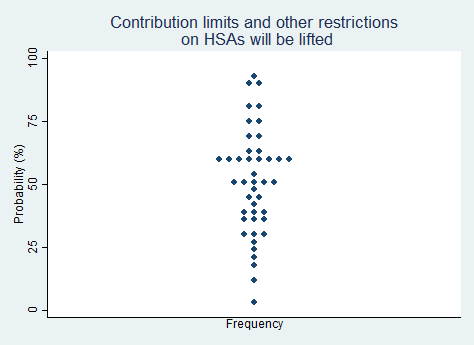
Proposition 28.
"Contribution limits and other restrictions on Health Savings Accounts (HSAs) will be substantially lifted."
2025 Median prediction: 50% prob (n = 44)
2024 Median prediction: 37% prob (n = 50)
Health Savings Accounts (HSAs) are tax-advantaged savings accounts designed to help individuals save for medical expenses. To be eligible for an HSA, individuals must have a high-deductible health plan (HDHP). Contributions to the account are tax-deductible, with funds growing tax-free and withdrawals for qualified medical expenses also tax-free. HSAs have been increasingly recognized as a tool for both short-term healthcare expenses and long-term savings, as unused funds roll over year after year and can even be used to save for retirement healthcare needs. Despite these advantages, HSAs are subject to contribution limits and other restrictions on how the funds can be used. These rules are set by the Internal Revenue Service (IRS).
There is potential political support for lifting these restrictions. Supporters argue that increasing contribution limits would allow individuals to save more for their medical expenses, providing them with greater financial flexibility and encouraging personal responsibility. Critics argue that higher contribution limits could disproportionately benefit wealthier individuals. Respondents in our survey are evenly split over the likelihood of the proposition that HSA contribution limits and other restrictions will be lifted in the next five years.
Conclusion
This forecasting exercise provides a snapshot of expectations regarding the future of U.S. health policy, with the aim of informing strategic planning and fostering more realistic discussions about the challenges and opportunities ahead. This is the second time we have undertaken this research project, and we intend to continue this project annually. Highlights from this year's findings include:
Policy changes rated as more likely to happen in the next five years:
- The share of U.S. healthcare spending will rise above 20% of U.S. GDP (76%)
- The federal government will reschedule or deschedule marijuana (60%)
- Substantial migration of physicians into Direct Primary Care (DPC) practices (50%)
- Substantial rise in direct-pay, cash-only ambulatory surgical centers (50%)
- At least several states will legalize the use of psychedelics for medical use (50%)
- Contribution limits and other restrictions on HSAs will be lifted (50%)
- Substantial shift toward price transparency tools to shop for care (50%)
Policy changes rated as least likely to happen in the next five years:
- We will experience another global pandemic like the COVID-19 pandemic (10%)
- The U.S. will adopt some form of Medicare For All, replacing private insurance (10%)
- Possible for workers to opt out of paying the Medicare tax and forgo Medicare (7%)
- A federal ban on abortion will be instituted (5%)
- Overall government spending on Medicaid will be lower than it is today (5%)
- Physician aid in dying will become legal in all fifty states (1%)
The three propositions with the biggest gain in probability over last year's survey were migration of physicians into DPC practices (+20 percentage points); lifting of HSA limits (+13 percentage points); and use of price transparency tools (+12 percentage points). The two propositions with the biggest decline in probability were reimportation of prescription drugs (-10 percentage points) and mandated paid sick leave (-10 percentage points). Like you, we look forward to seeing how the landscape changes.
References:
1. Mannes, A. E., Soll, J. B., & Larrick, R. P. (2014). The wisdom of select crowds. Journal of Personality and Social Psychology, 107(2), 276—299.
2. Brooks, David. "How the Ivy League Broke America." The Atlantic. November 14, 2024.
3. Navajas, J., Niella, T., Garbulsky, G. et al. Aggregated knowledge from a small number of debates outperforms the wisdom of large crowds. Nat Hum Behav, 126-132 (2018).